[1] Hedegaard, M., Warner, M., & Minino, A. M. (2017, December). Overdose deaths in the United States, 1999-2016. NCHS Data Brief, 294. US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics. Available: https://www.cdc.gov/nchs/data/databriefs/db294.pdf
[2] Florida Drug-Related Outcomes Surveillance and Tracking System (FROST), University of Florida College of Medicine. http://frost.med.ufl.edu/frost/
[3] The National Center on Addiction and Substance Abuse at Columbia University. (2011). Adolescent Substance Use: America’s #1 Public Health Problem. New York, NY: Author. Available: https://www.centeronaddiction.org/addiction-research/reports/adolescent-substance-use-america%E2%80%99s-1-public-health-problem
[4] DuPont, R. L., Han, B., Shea, C. L., & Madras, B. K. (2018). Drug use among youth: national survey data support a common liability of all drug use. Preventive Medicine, 113, 68-73.
[5] DuPont, R. L. (2015). It’s time to re-think prevention: increasing percentages of adolescents understand they should not use any addicting substances. Rockville, MD: Institute for Behavior and Health, Inc.
[6] DuPont, R. L. (2017, October 23). For a healthy brain teens make “One Choice”. Rockville, MD: Institute for Behavior and Health, Inc. Available: https://www.preventteendruguse.org/s/IBH_Commentary_One_Choice_10-23-17.pdf
[7] Chadi, N., & Levy, S. (2017). Understanding the highs and lows of adolescent marijuana use. Pediatrics, 140(6). Available: http://pediatrics.aappublications.org/content/pediatrics/early/2017/11/02/peds.2017-3164.full.pdf
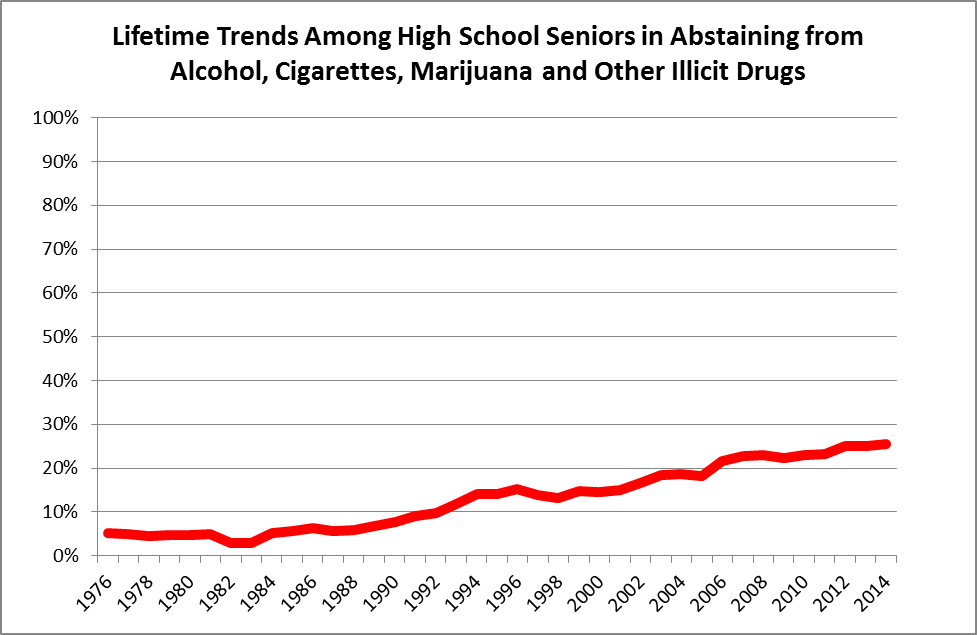
[8] Levy, S., Campbell, M. C., Shea, C. L., & DuPont, R. L. (2018). Trends in abstaining from substance use in adolescents: 1975-2014. Pediatrics, doi: 10.1542/peds.2017-3498.
[9] Miech, R. A., Johnston, L. D., O’Malley, P. M., Bachman, J. G., Schulenberg, J. E., & Patrick, M. E. (2017). Monitoring the Future national survey results on drug use, 1975–2016: Volume I, Secondary school students. Ann Arbor: Institute for Social Research, The University of Michigan. Available at http://monitoringthefuture.org/pubs.html#monographs
[10] Dufton, E. (2017). Grass Roots: The Rise and Fall of Marijuana. New York, NY: Basic Books.
[11] Geiger, A. (2018, January 5). About six-in-ten Americans support marijuana legalization. Washington, DC: Pew Research Center. Available: http://www.pewresearch.org/fact-tank/2018/01/05/americans-support-marijuana-legalization/
[12] Caulkins, J. (2017, November 7). Psychoactive drugs in light of libertarian principles. Law and Liberty. Available: http://www.libertylawsite.org/liberty-forum/psychoactive-drugs-in-light-of-libertarian-principles/
[13] ElSohly, M. A., Mehmedic, Z., Foster, S., Gon, C., Chandra, S., & Church, J. C. (2016). Changes in cannabis potency over the last 2 decades (1995-2014): Analysis of current data in the United States. Biological Psychiatry, 79(7), 613-619.
[14] World Health Organization. (2016). The Health and Social Effects of Nonmedical Cannabis Use. Geneva, Switzerland: Author. Available: http://www.who.int/substance_abuse/publications/cannabis/en/
[15] Rocky Mountain High Intensity Drug Trafficking Area. (2017, October). The Legalization of Marijuana in Colorado: The Impact, Volume 5. Denver, CO: Author. Available: https://rmhidta.org/files/D2DF/2017%20Legalization%20of%20Marijuana%20in%20Colorado%20The%20Impact2.pdf
[16] E.g., Sanger-Katz, M. (2018, August 16). Bleak new estimates in drug epidemic: a record 72,000 overdose deaths in 2017. The New York Times, p. A1. Available: https://www.nytimes.com/2018/08/15/upshot/opioids-overdose-deaths-rising-fentanyl.html; Seelve, K. Q. (2018, January 21). One son. Four overdoses. Six hours. A family’s anguish. New York Times, p. A1. Available: https://www.nytimes.com/2018/01/21/us/opioid-addiction-treatment-families.html
[17] Drug Policy Alliance. (2018). Real drug education. New York, NY: Author. Available: http://www.drugpolicy.org/issues/real-drug-education
[18] The President’s Commission on Combatting Drug Addiction and the Opioid Crisis. (2017). Final Draft Report. Available: https://www.whitehouse.gov/sites/whitehouse.gov/files/images/Final_Report_Draft_11-15-2017.pdf